Breast Implant Removal & Capsulectomy
There are various reasons some patients choose to have their breast implants removed, and Dr. McInnes is knowledgeable and skilled at helping these patients. Much like information about vaccines, allergies, and various diets, there is an exceptional amount of information about breast implants online, some true, but much of it false. Dr. McInnes is well-educated about breast implants, their risks, new trends, and risks of implant removal. He is a caring physician and, like all surgeries he performs, wants his patients to understand the objective facts of their surgery, and assist them in making well-informed decisions. Dr. McInnes’ first priority is, by far, safe implant removal without damaging critical structures. Knowledge and data on breast implants is expanding, and therefore guidelines and recommendations are also subject to change.
En-bloc vs. total capsulectomy vs. “standard” implant removal…what’s the difference?
After a foreign object enters the body (such as a breast implant, an artificial joint, a prosthetic cardiac value, or a sliver) the body’s immune system will form a layer of scar tissue around it and “wall it off” from the rest of the body. Essentially, breast implants will have an outer shell formed by the body called a capsule. This capsule can be removed at the time of implant removal.
Complete capsulectomy (aka total capsulectomy) refers to removing all of the capsule that forms around the implant, which can be achieved with either an en-bloc technique or the more traditional method of implant removal. Many women wanting their implants removed are also wanting complete capsulectomy. Please note, a complete capsulectomy does not provide a 100% guarantee that some type of implant-associated pathology will not develop in the future.
Book Your Consultation
En-bloc technique involves removing the implant without violating this tissue capsule. This technique is preferable in circumstances such as implant rupture or ALCL, but many patients are now requesting this for regular implant removal. Traditionally, most implants have been removed by incising the implant capsule and removing the implant, followed by part of the capsule. That approach can be done through a smaller incision. Both techniques have the potential to remove the entire capsule, however en-bloc technique requires a larger incision and scar, takes more operative time, and has a steeper learning curve from a surgical standpoint. Just because an implant has been removed en-bloc, this does not guarantee a complete capsulectomy. There can be a double capsule, and additional capsular remnants in the breast cavity that are no longer fixated to the main capsule. For a complete capsulectomy, this requires the cavity to be diligently inspected after the implant is removed. Similarly, even if a diligent surgeon believes they’ve perfomed a complete capsulectomy, they cannot 100% guarantee that some small, non-visible section of capsular cells were not left behind.
Please note, no surgeon can guarantee they won’t inadvertently puncture or tear part of the capsule during an attempted en-bloc removal, which essentially defeats the purpose. In fact, several American surgeons whose entire practice is implant removal have stated they’re successful at en-bloc (ie. not a single capsular tear) about 25% of the time. En-bloc removal is facilitated by a thick capsule, but if the capsule is exceedingly thin, such as a single layer of wet tissue paper, then it’s almost impossible to remove it en-bloc. For modest capsules, there are certain techniques Dr. McInnes has incorporated which improve the chances of the implant coming out 100% en-bloc, and also improve safety. To date, the benefit of en-bloc implant removal in the setting of an intact implant (non-ruptured) without ALCL is only theoretical. In many internet circles, the en-bloc technique is described as the gold standard in all situations, however this is not necessarily the case. Having now performed many successful en-bloc implant removals, Dr. McInnes does feel it can often be done safely, particularly with the safety measures he takes. That being said, there have been reports of pneumothorax, exposed pericardium, and extensive bleeding occurring with the en-bloc technique. It is only a matter of time before there are reports of nerve damage from implant removal. Make no mistake, those are real risks with real implications, and non-surgeons on internet forums do not have a true appreciation for surgical risks. This is much less of an issue with implants placed above the muscle, as those placed below the muscle tend to have capsules that are adherent to the outer layer of the ribs. It is unclear if all surgeons performing complete capsulectomy consider an adherent posterior capsular wall part of the capsule or part of the ribs. Removing this part of the capsule is not always done by all surgeons. Whether it’s removal is considered part of a complete capsulectomy may depend on the surgeon. The benefit of removing this part of the capsule in the setting of smooth walled implants, much like the rest of the capsule, has not been established or validated in the scientific medical literature. Like BII in general, it would be a tremendous undertaking to study that aspect of complete capsulectomy. Dr. McInnes will discuss the removal of the posterior capsule with you at your consultation so you are aware of the risks involved with its removal, and other available options if it is very stuck down (ie. plan B).
How does Dr. McInnes perform en-bloc implant removal?
Dr. McInnes has extra fellowship training (ACGME-accredited) in microsurgery and peripheral nerve surgery, giving him expert-level ability to make the surgery as safe as possible. He incorporates these skills and uses new-generation surgical headlighting while meticulously removing the capsule. These are all safety measures aimed to minimize the chances of bleeding if the capsule needs to be removed off the ribs. Dr. McInnes does his absolute best to minimize any bleeding during surgery. He is fully aware of the proximity an implant capsule can have to the lung and nerves, and very carefully and meticulously removes it in those areas. Through experience, Dr. McInnes has also developed a technique for safely removing the most superior part of the implant which he can explain at your consultation.
What might decrease the chance of my implant being removed en-bloc?
- Thin capsules make it much more difficult as they often don’t hug as tightly around the implant and they easily tear.
- “loose” capsules: some capsules extend much farther superiorly than the resting position of the implant. If capsules are very loose they can ride up over the pectoralis minor muscle, which partially covers the nerves that move the arm.
- Previous axillary incision for implant placement: the capsules are often long going high into the axilla which is a surgical danger zone with respect to critical nerves.
- Adherence to the ribs: Dr. McInnes can remove the outer periosteal layer of the rib for an attempted en-bloc surgery, but if highly adherent it can easily tear. An analogy might be peeling off wet tissue paper that has been glued down to a hard surface…very easy to tear. If the capsule has thickened and contracted, removing it en-bloc is actually much easier.
Does Dr. McInnes give a 100% guarantee to remove all capsule?
- In practice, this is almost always the case and it’s certainly his expectation, but for patient safety purposes, he doesn’t make this promise, and feels it’s unsafe for any surgeon to make this guarantee. He welcomes any questions about this during your consultation.
If he always performs a complete capsulectomy, why not commit to it 100%?
- In theory the capsule could be stuck down to the nerves that move the arm, or be so stuck to the ribs that removing it could cause a pneumothorax (which has a risk of death). There are certain anatomic factors that can only be identified during surgery, and the most important goal of implant removal is SAFE implant removal. Dr. McInnes is very meticulous and mentally commits to complete capsulectomy for each case, but he won’t compromise patient safety if required (and no surgeon should!).
What happens if I have a ruptured implant and it doesn’t come out en-bloc?
- If this happens, Dr. McInnes has a very reliable sequence of clearing out the pocket of any silicone. If possible, he will re-staple the capsule to seal it off and proceed with the surgery. If this is not possible, he will drape right around the capsule tear within your breast. He will then use a large suction device and remove the implant and it’s contents which usually come out nicely. He will then aggressively flush out the pocket, complete the capsulectomy, and re-flush the pocket with antibiotic solution. The pocked is almost always completely clean and devoid of any silicone.
What can I expect after surgery?
After implant removal, you will likely have drains to keep the breast tissue stuck down so it heals nicely. This also helps minimize the chance of fluid buildup where the implant used to be. Dr. McInnes will give you antibiotics while you have drains in place to minimize your chance of infection, and appropriate pain killers.
Pictures, special tests, etc
Generally speaking, Dr. McInnes is fine with most special requests, but they must be discussed at the time of consultation, before the day of surgery. He is willing to take photos, within reason. En-bloc implant removal requires a fair amount of concentration during the operation, and Dr. McInnes does not want to be overly distracted with extensive image requests while operating.
Do I need a breast lift (mastopexy) after my implant removal?
Breast implants do thin out some of the breast tissue, stretch the skin, and after implant removal can leave a sagging appearance to the breast tissue. In some cases, this skin and tissue with contract enough that a breast lift procedure is not necessary. Dr. McInnes will recommend an immediate breast lift if he thinks it will actually be required to match your aesthetic goals. Many patients have been pleasantly surprised after implant removal, and decided not to proceed with the breast lift component. There are advantages and disadvantages to staging the breast lift procedure, and Dr. McInnes will discuss these with you at your consultation. He will also give his opinion as to whether he thinks it’s best you perform an immediate breast lift, a staged breast lift, or no breast lift. Each case is different and depends on numerous factors. Fat grating may also be utilized to reconstitute some of the volume loss from implant removal.
His office said he won’t remove my implants, why not?
Due to his extensive practice and limited availability, patients wanting non-private (ie. MSP covered) implant removal are encouraged to see their original implant surgeon or their direct successor if retired. Dr. McInnes has limited his implant removal practice to private cases or those with combined private procedures.
What are the risks of implant removal with complete capsulectomy?
Implant removal is real surgery, and regardless of what any surgeon or non-surgeon says, there are inherent risks to the operation. The following are risks for every surgeon performing this procedure, although the likelihood of many of these risks very low. The most common would be bruising, infection, and seroma (fluid buildup in the breast). By taking this surgery seriously and performing it in an accredited surgical facility, and having the necessary training and experience with this operation, Dr. McInnes is confident in your safety. He reiterates that implant removal and complete capsulectomy is a personal choice, but in most circumstances, professional plastic surgery societies and Health Canada do not recommend prophylactic surgery (ie. surgery for patients without an objectively established medical diagnosis).
Risks for en-bloc implant removal include, but are not limited to:
- Larger scars
- No guarantee of symptom resolution
- Infection
- Pain
- Bruising
- Bleeding and need for drainage
- Seroma
- Nerve injury (sensory nerves, brachial plexus)
- Need to remove a segment of rib (for bleeding)
- Tension pneumothorax (air leak around lung)
- Breast asymmetry
- Nipple sensory changes
- Nipple and skin necrosis
- Breast deformity
- Need for revisional surgery
- Asymmetric breast contracture post-operatively
- Need/want for a post-operative mastopexy (breast lift)
- No guarantee 100% capsule removal if puts a patient at risk for a significant complication
- No guarantee of 100% en-bloc removal technique if tearing occurs in the capsule
- Difficulties with breast feeding
- Deep vein thrombosis/ pulmonary embolism (can cause death)
Breast Implant Removal Cost in Vancouver
The cost of a breast implant removal in Vancouver is based on individual surgical requirements and the exact procedures you require will be provided after your consultation. An Implant removal, full capsulectomy (attempted en-bloc) starts at $13,000, and includes a lift for $17,000 and a lift & fat grafting for $21,500+. Financing plans are available and are an increasingly popular option.
Questions?
Every implant removal case is different, and Dr. McInnes is happy to meet with you to discuss the operation and answer your questions.
There are risks associated with your surgery. Please download the consent form designed by the American Society of Plastic Surgeons (ASPS) for a detailed list and description of the risks involved (found here). Risks of surgery will be discussed prior to your consent. It is important to address all your questions directly with Dr. McInnes.
En-bloc Capsulectomy (operative photos)
Click on the photo below to view more photos
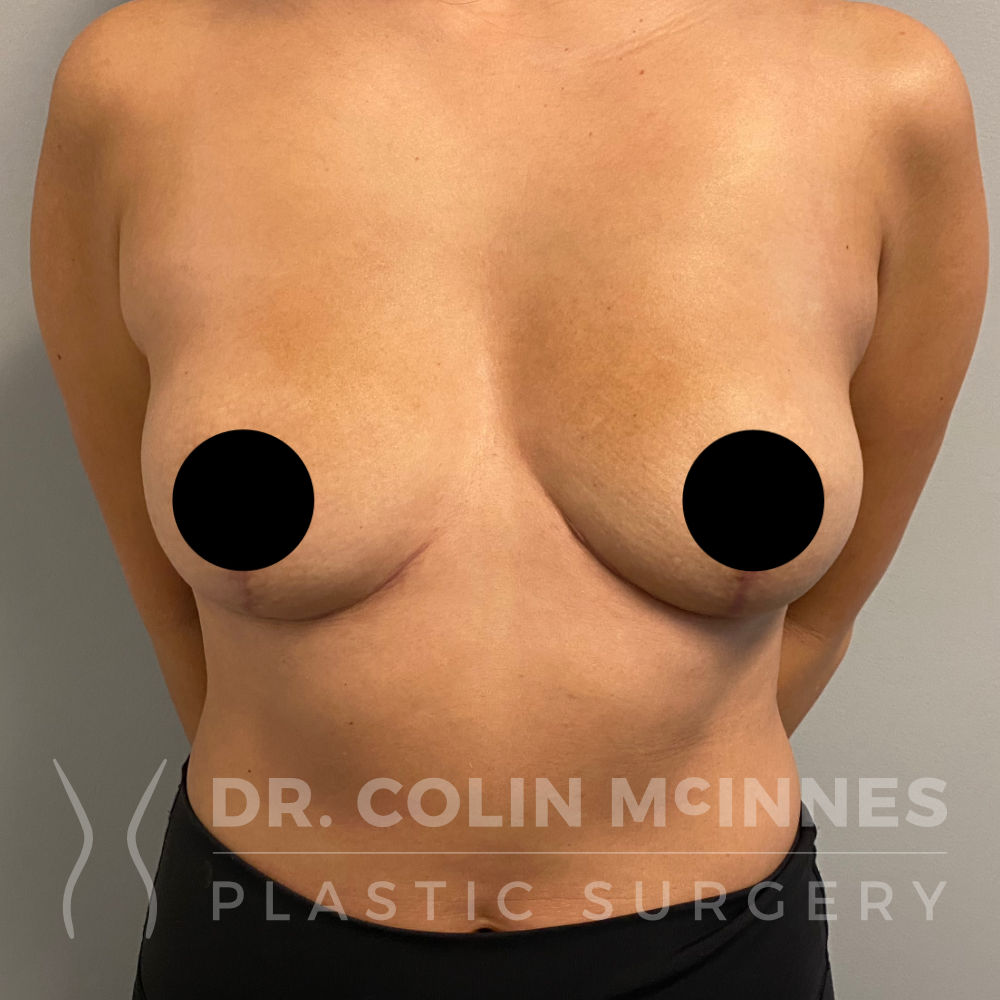
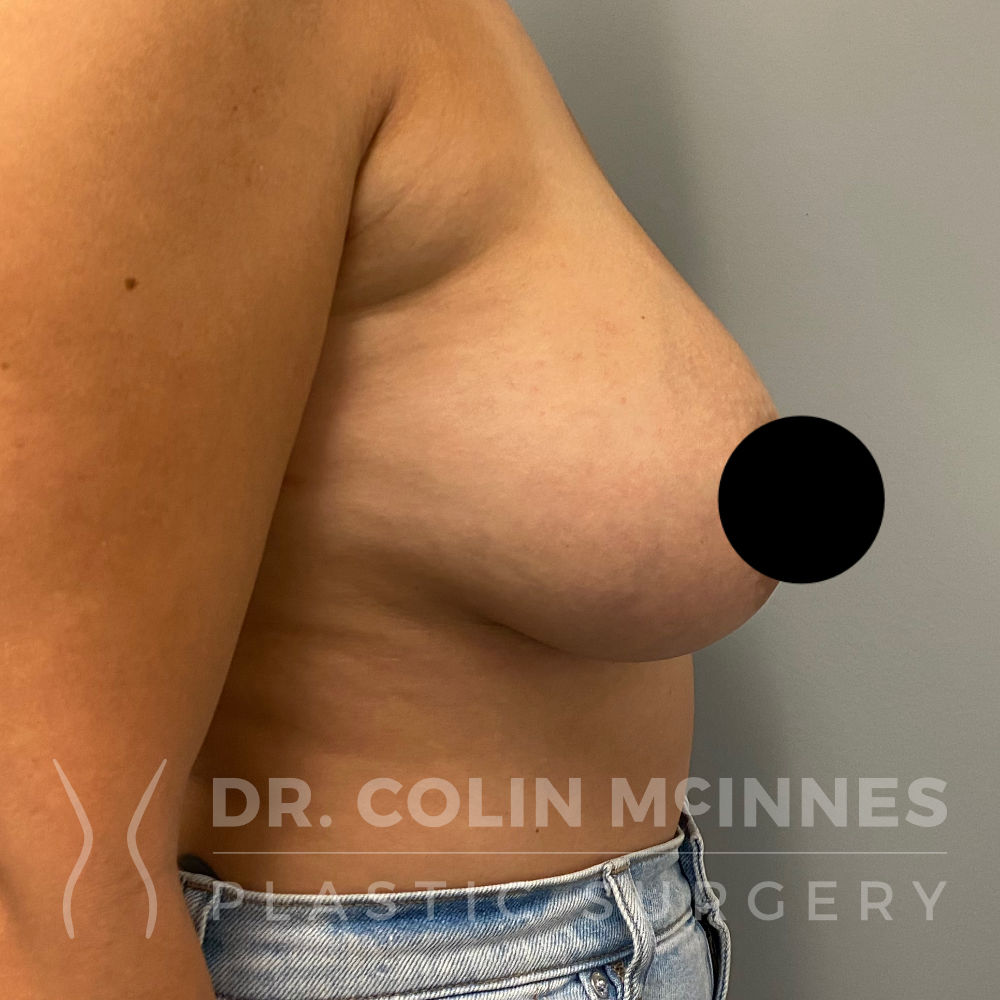
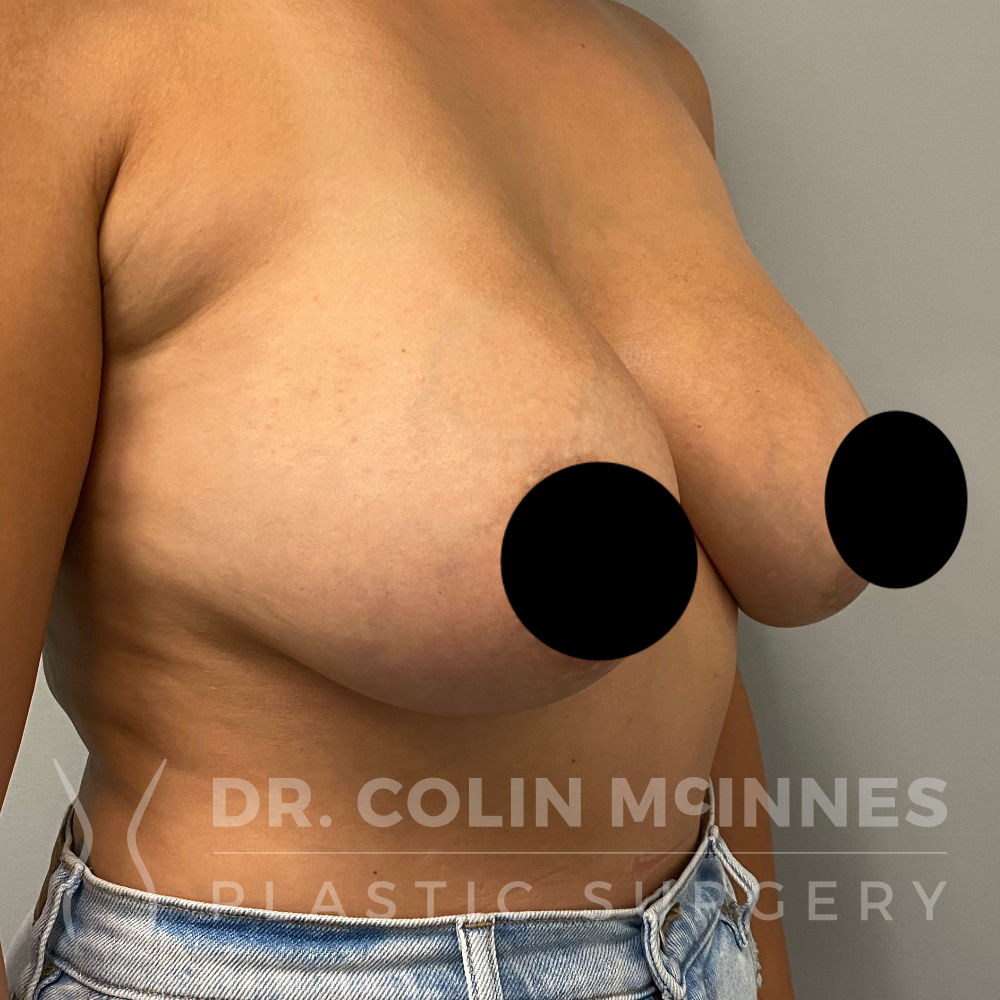
Before & After Photos
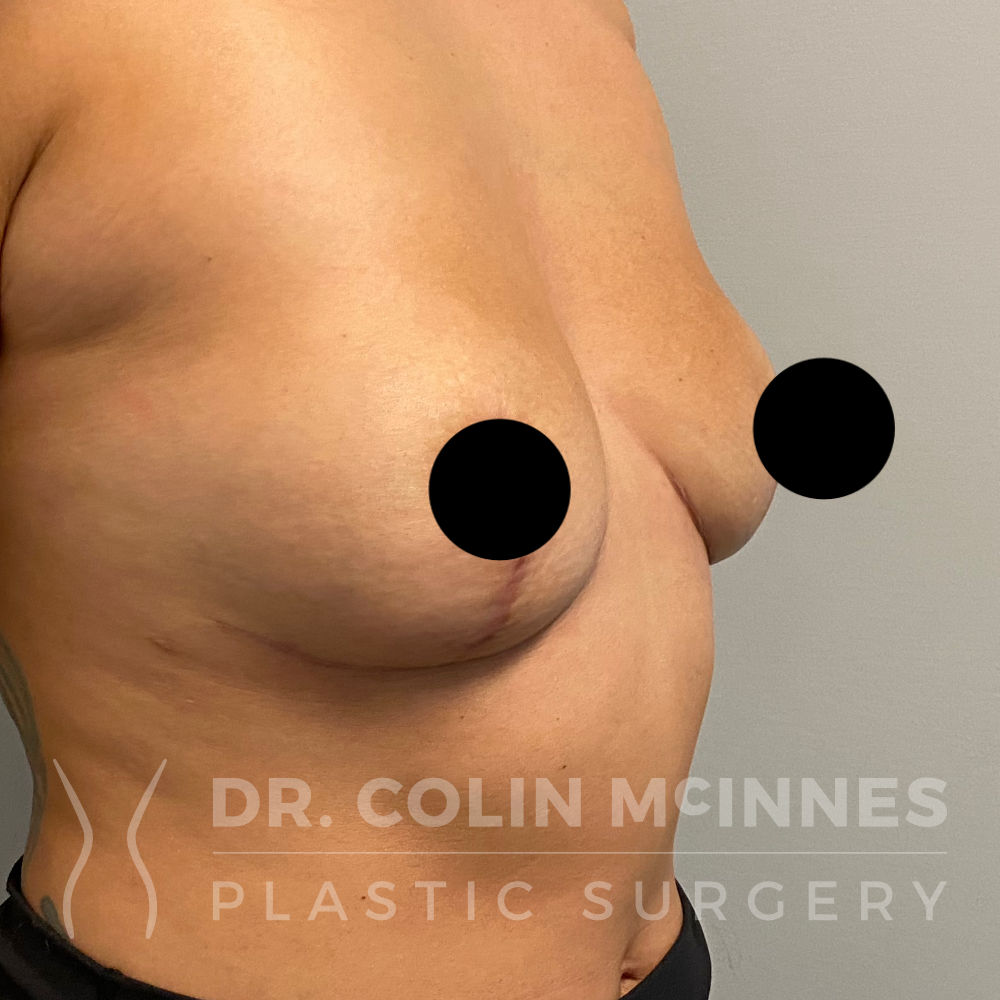
Implant Removal / Capsulectomy & Immediate Lift
Before

6 months post-op
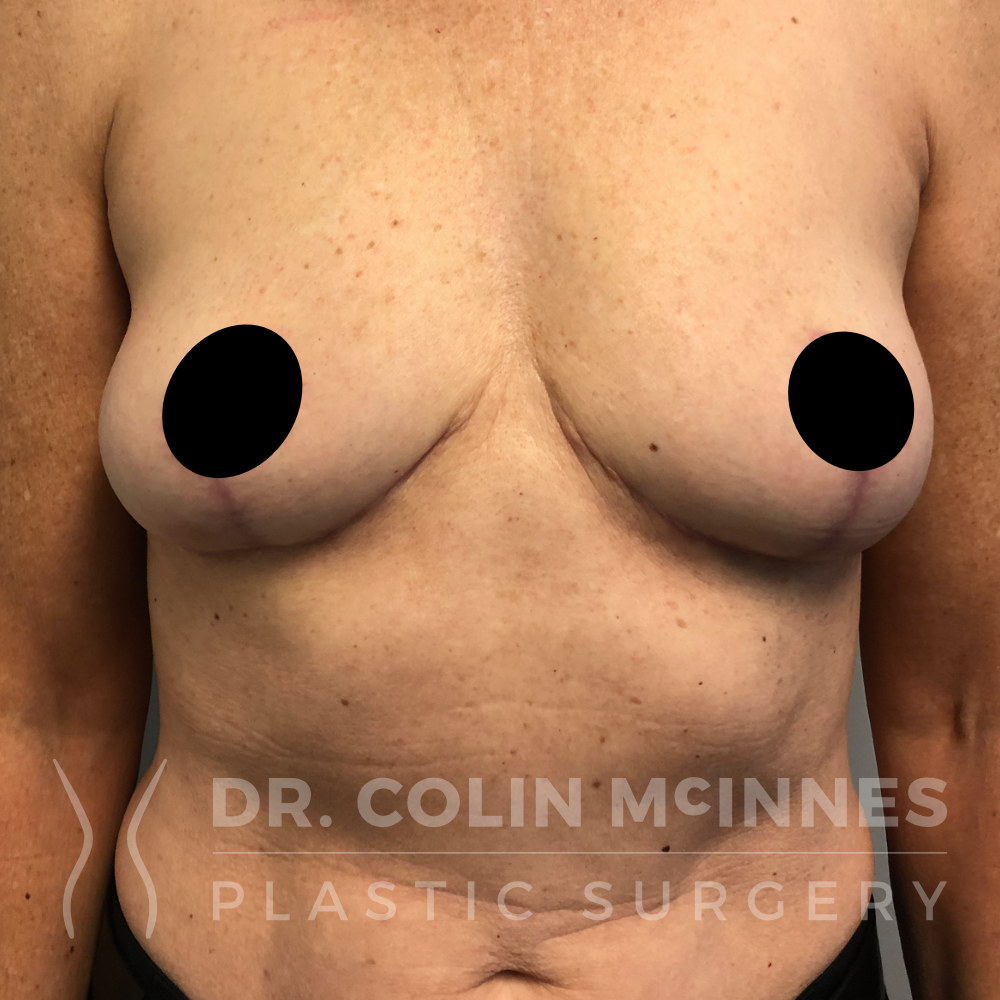
Explant with Immediate Breast Lift
Before
3 months post op
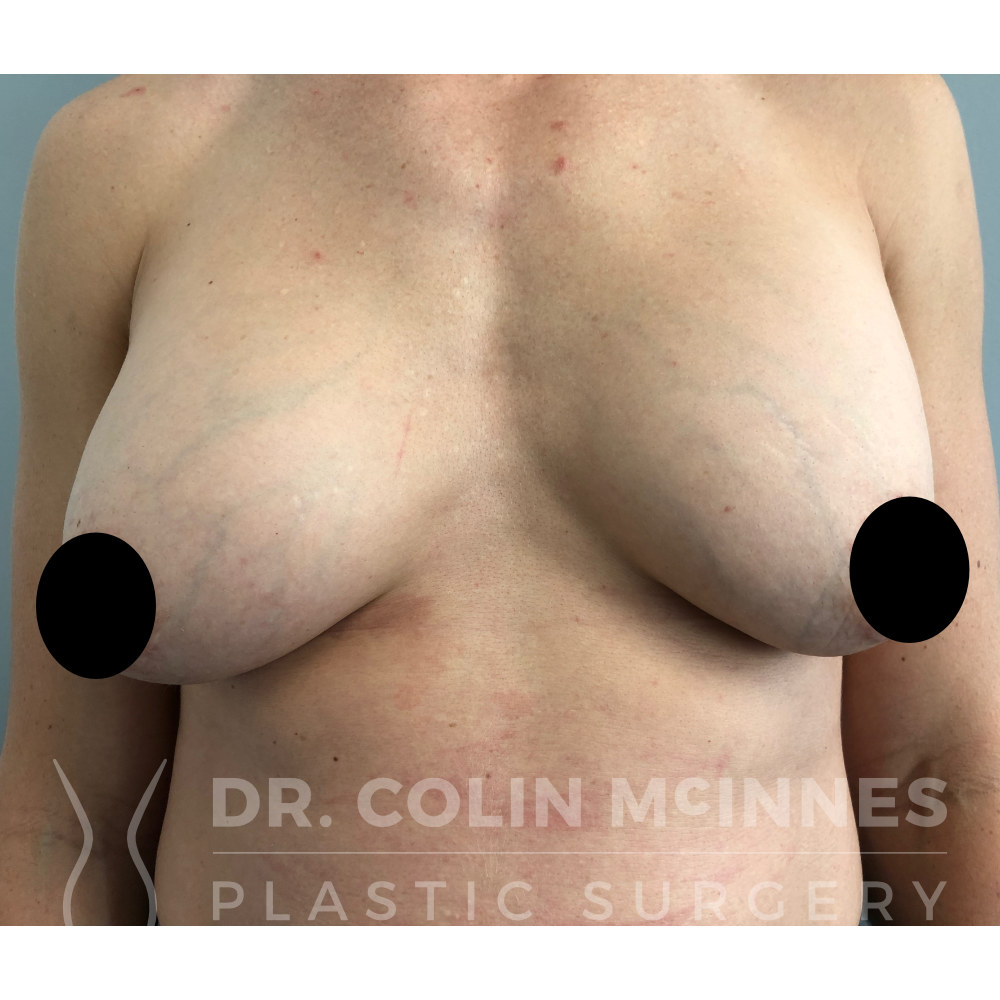
En-Bloc Explant with Immediate Breast Lift
Before
4 months post op

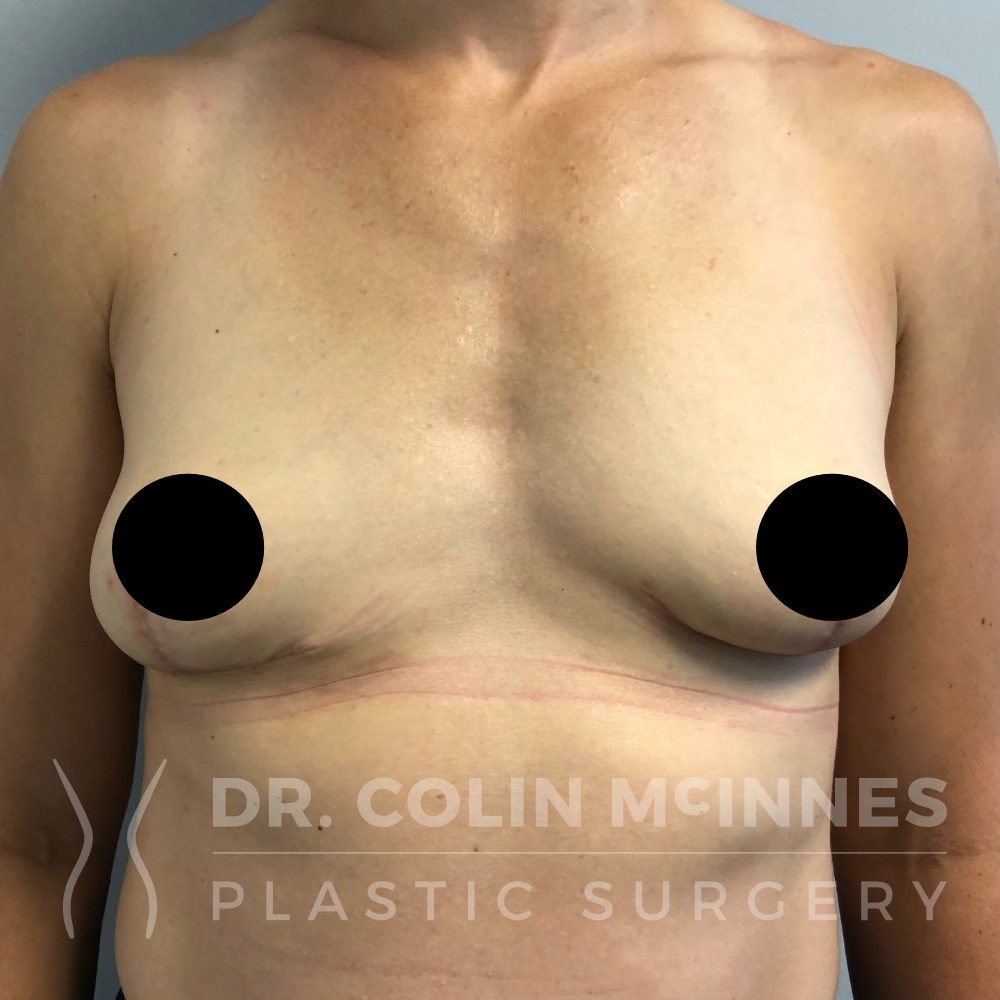
En-Bloc Explant with Immediate Breast Lift
Before
4 months post op
En-Bloc Explant with Immediate Breast Lift
Before

4 months post op